Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19
76-year-old man with Parkinson's disease (PD) died three weeks after receiving his third COVID-19 vaccination, 5 months after his second dose (BNT162b2 mRNA vaccine/Comirnaty) and 7 months since his first dose (ChAdOx1 nCov-19 vector vaccine).
On the day of his first vaccination, the individual experienced pronounced cardiovascular side effects, for which he repeatedly had to consult his doctor. After the second vaccination two months later, the family noted obvious behavioral and psychological changes (e.g., he did not want to be touched anymore and experienced increased anxiety, lethargy, and social withdrawal even from close family members). Furthermore, there was a striking worsening of his PD symptoms, which led to severe motor impairment and a recurrent need for wheelchair support. He never fully recovered from these side effects after the first two vaccinations but still got another vaccination in December 2021. Two weeks after the third vaccination, he suddenly collapsed while taking his dinner. Remarkably, he did not show coughing or any signs of food aspiration but just fell down silently. He recovered from this more or less, but one week later, he again suddenly collapsed silently while taking his meal. The emergency unit was called, and after successful, but prolonged resuscitation attempts (over one hour), he was transferred to the hospital and directly put into an artificial coma but died shortly thereafter. The clinical diagnosis was death due to aspiration pneumonia. There was no history of a clinical or laboratory diagnosis of COVID-19 in the past.
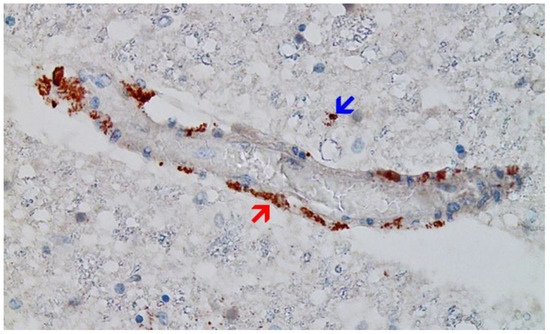
The family of the deceased requested an autopsy due to ambiguous clinical signs before death. Histopathological analyses of the brain uncovered previously unsuspected findings, including acute vasculitis (predominantly lymphocytic) as well as multifocal necrotizing encephalitis of unknown etiology with pronounced inflammation including glial and lymphocytic reaction. In the heart, signs of chronic cardiomyopathy as well as mild acute lympho-histiocytic myocarditis and vasculitis were present. Although there was no history of COVID-19 for this patient, immunohistochemistry for SARS-CoV-2 antigens (spike and nucleocapsid proteins) revealed only spike protein but no nucleocapsid protein within the foci of inflammation in both the brain and the heart, particularly in the endothelial cells of small blood vessels. The figure shows one example of the abundant presence of SARS-CoV-2 spike protein in swollen endothelium of a capillary vessel. Since no nucleocapsid protein could be detected, the presence of spike protein must be ascribed to vaccination rather than to viral infection. The findings corroborate previous reports of encephalitis and myocarditis caused by gene-based COVID-19 vaccines.
Several autopsy reports of vaccinated individuals have been published in medical literature or discussed in the media. Examples are cases of a 28-year-old Bangladeshi man, an 86-year-old man, and 54 Japanese individuals.
REFERENCE
Mörz M. A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19. Vaccines (Basel). 2022 Oct 1;10(10):1651. doi: 10.3390/vaccines10101651. PMID: 36298516; PMCID: PMC9611676.



Comments
Post a Comment